
Cure SMA: Evaluation of SMA in the Era of Telehealth - Episode 6
Use of Telehealth to Address Parental Concerns
Garey H. Noritz, MD, stresses the value of in-person office visits for babies to ensure they receive their vaccinations and physical examination.


Diana Castro, MD: Now we’re living with COVID-19. I’m sure things have changed for you because they have changed for all of us. How can providers conduct developmental screening within a telehealth environment to address the parental concerns regarding their children’s motor developmental capacities? Is there anything you recommend or try for the families to help them?
Garey H. Noritz, MD: There is a little bit of a two-pronged approach. One is that we believe that what we do in the office—even though there is more risk coming to the office than staying home—is beneficial because we can do a better exam, we can give immunizations that the child needs, and we can talk in person, which is better than talking over Zoom. We’ve created systems within our offices to minimize as much of the risk as we can of any COVID-19 transmission. But I completely understand not wanting to bring your precious new baby into the world that seems so scary right now.
Part of it is giving the message that it’s really OK and it’s important to do these things. Telehealth has its place, but in early childhood general pediatrics, it’s so important to get them in for immunizations and examination, because that’s where we’re going to pick up things like a heart murmur, weakness, a hearing problem, or anything unexpected. If it were expected, we wouldn’t need to bring you to the office. There’s that part of it.
The other part of it is that from here on out, we’re always going to be doing some amount of telehealth. It’s a matter of making this interaction fruitful for both the family and for the pediatricians to say, “Are we meeting the family’s needs to talk to the doctor, ask their questions about their child, hear about what’s coming up in the child’s development, express their concerns, and so on?” It’s also our job to look at the child and say, as best as we can in a remote environment, “This child really looks like they’re doing very well. I don’t see any signs of weakness. I don’t see any signs of developmental delay. I don’t see anything that makes me concerned about other kinds of diseases.”
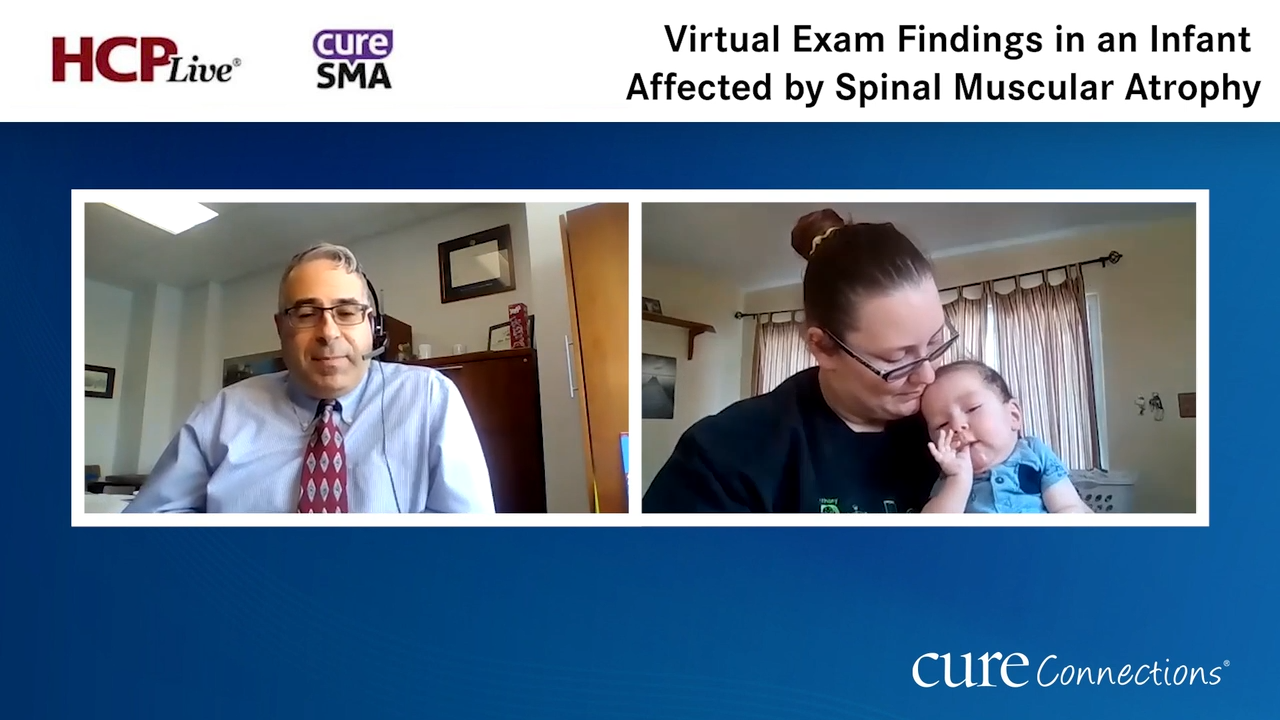
A lot of the exam is done visually, and we don’t even realize we’re doing it as pediatricians. We sit, we come in, we talk to the family, the child is sitting on the parent’s lap, and we’re watching that interaction. We learn so much from that interaction. We see how they hold themselves, how they move their arms, how they move their legs, and how they breathe. We can do that on video. What we can’t do is feel the baby in our hands, and that is incredibly key. When I work with pediatric residents, I tell them, “Pick up every baby you see because that’s how you understand what a baby feels like. Then you’ll know when a baby doesn’t feel right, and you can go from there.”
There are other things we’re going to look for. We’ll want to check for deep tendon reflexes. We can’t really do that over video. Maybe you can walk the family through it, but it’s not the same as doing it yourself. Maybe the video is good enough that you can see fasciculations in the tongue. But that’s somewhat hard to see, and we’ve got a parent who’s trying to talk, hold the baby, and be the cameraman at the same time. That makes it really tough to see as much as you can.
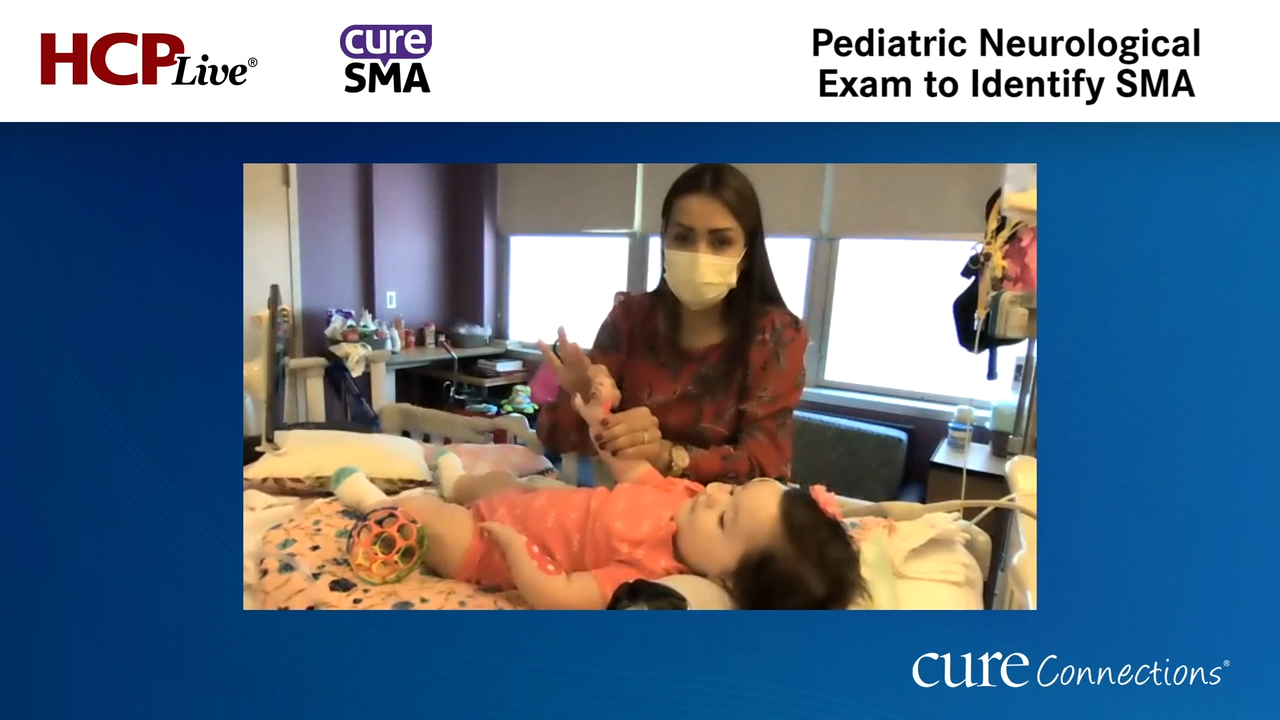
If I wanted to look at a baby and be convinced this child doesn’t have SMA [spinal muscular atrophy], what I would just do is have them strip the baby down to the diaper and let me watch them lay on their back. It would let me see them move their arms and legs, breathe, and move their head. To some extent, it doesn’t matter what age they are because we can see things that suggest SMA or weakness: a small chest, a bell-shaped chest, wasting of the muscles, not much movement against gravity—those kinds of things, as well as how interactive the baby is and how expressive they are in the face, which we said is a hallmark of SMA. This is not going to replace seeing people in the office.
Diana Castro, MD: You do immunizations. During this COVID-19 situation, your patients are still coming to get those immunizations at 2 months, 4 months, 6 months, and so on. That’s key for the ones with infantile onset because you have the opportunity to have that baby in front of you at 2, 4, and 6 months. It’s key to look for all those things that you were describing.
Garey H. Noritz, MD: For sure, and we would never want a baby with SMA to get pertussis. That is very bad for them.
Diana Castro, MD: Exactly.
Dr Noritz, thank you so much. It was a very interesting conversation. Thank you for watching this HCPLive® Cure Connections® program. If you’re enjoying the content, please subscribe to our e-newsletter to receive upcoming programs and other great content in your inbox. Thank you so much.
Garey H. Noritz, MD: Thank you.
Transcript Edited for Clarity


